INSPIRED BY PATIENTS, DRIVEN BY SCIENCE.

-
![]()
City skyline
Photo By: John DoeButton
DR. ANAHID JEWETT
THANK YOU FOR VISITING OUR WEBSITE...
Cure Cancer Now Foundation was organized by a diverse group of very distinguished and internationally recognized scientists engaged in many types of cancer research. Through our relentless efforts and successes, we realized that to expedite cancer cures, increased funding and private sector philanthropy is vital and urgently needed.
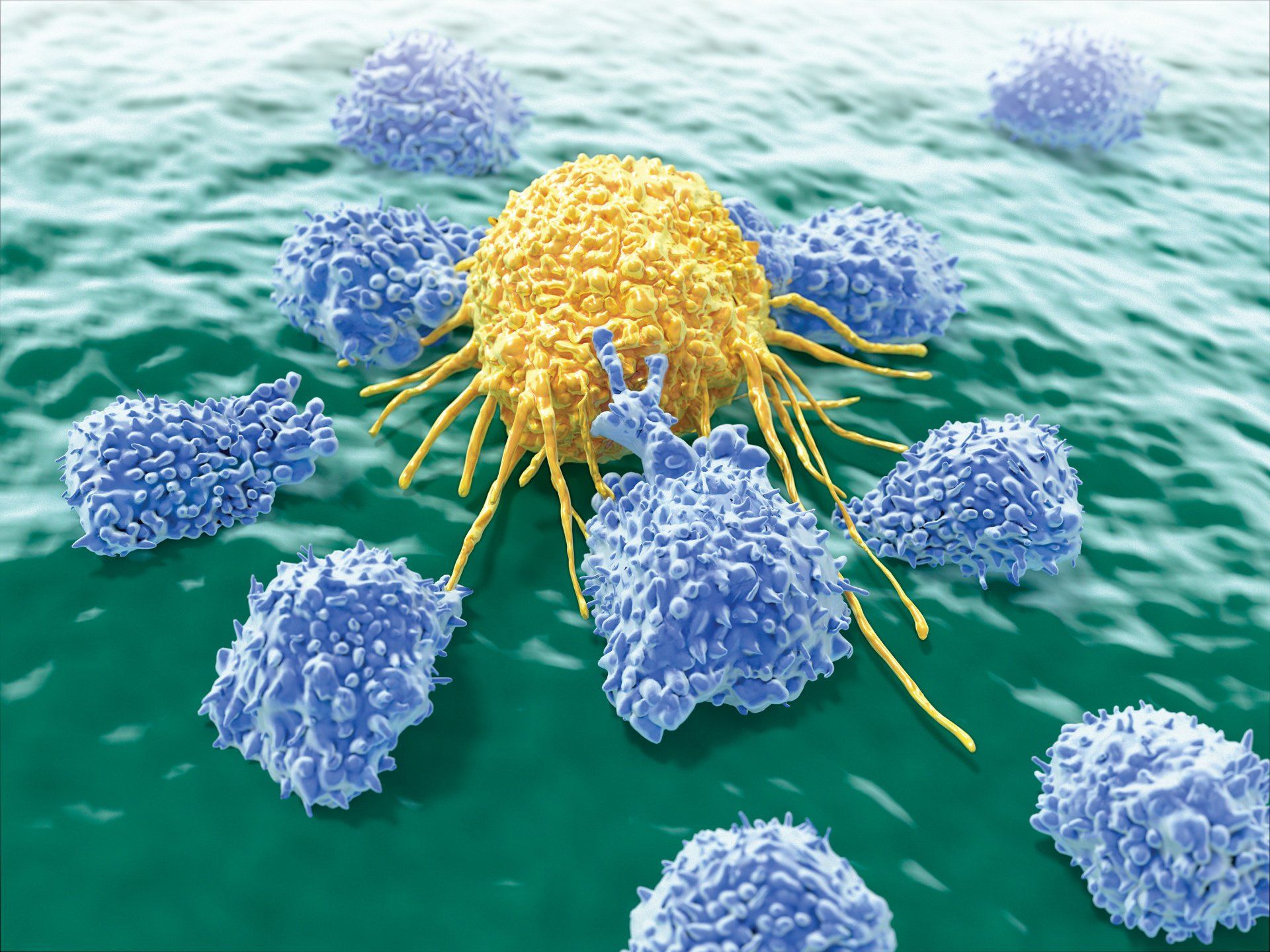
Cancer is an extremely challenging disease caused by many factors, including:
- Mutations that inhibit oncogene and tumor suppressor gene function, leading to uncontrollable cell growth
- Carcinogens that damage DNA, promoting or aiding cancer. Examples of carcinogens are tobacco, environmental exposure to asbestos, arsenic, radiation, etc.
- Viruses – HPV, Hepatitis B & C, Epstein-Barr, HIV
- Genetic predisposition inherited from family members.
- Obesity
Worldwide in 2012 there were 14.1 million new cancer cases, 8.2 million cancer deaths and 32.6 million people living with cancer (within 5 years of diagnosis). 57% (8 million) of new cancer cases, 65% (5.3 million) of the cancer deaths and 48% (15.6 million) of the 5-year prevalent cancer cases occurred in the less developed regions.
The overall age standardized cancer incidence rate is almost 25% higher in men than in women, with rates of 205 and 165 per 100,000, respectively. Male incidence rates vary almost five-fold across the different regions of the world, with rates ranging from 79 per 100,000 in Western Africa to 365 per 100,000 in Australia/New Zealand (with high rates of prostate cancer representing a significant driver of the latter).
There is less variation in female incidence rates (almost three-fold) with rates ranging from 103 per 100,000 in South-Central Asia to 295 per 100,000 in Northern America.
In terms of mortality, there is less regional variability than for incidence, the rates being 15% higher in more developed than in less developed regions in men, and 8% higher in women.
In men, the rates are highest in Central and Eastern Europe (173 per 100,000) and lowest in Western Africa (69). In contrast, the highest rates in women are in Melanesia (119) and Eastern Africa (111), and the lowest in Central America (72) and South-Central (65) Asia.1
Cancer has many causes and the treatment choices vary considerably. These choices must be responsible and effective in order to maintain and/or restore a high quality level of health and physical function.
It is our mission to promote cancer research, thereby accelerating the development of effective cancer treatments.
There have been successes in the fight against cancer, but challenges remain and our work continues. We realize that the battle to overcome cancer can be achieved in part, by spreading cancer awareness, providing early detection and early treatment regimens, but most importantly through continued scientific research.
Pushing the boundaries of scientific research takes time and considerable financial resources. We triumph when we develop cures, made possible by your generous donations.
Thank you for your support of this worthy cause.
Dr. Merlin Williams
Ref: International Agency for Research on Cancer
World Health Organization
GLOBOCAN 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 20121
WHAT'S NEW AND EXCITING